

Redesigning the International Patient Services Experience
Timeline
March - December 2025 (10-months)
Role
Digital Product Designer
Tools
Figma, Aha!, Words, Excel, Photshop
Overview
Unclear service offerings and fragmented care pathways made it difficult for international patients to confidently navigate Mayo Clinic’s digital experience. This lack of clarity limited patients’ ability to act and created downstream inefficiencies for operational teams responsible for intake, routing, and support, highlighting the need for a more cohesive, patient-centered system.
Problem
Mayo Clinic’s International Patient Services digital experience was not aligned with how global patients research, evaluate, and access complex care. Low discoverability, fragmented pathways, and inconsistent content created confusion for non-native English speakers, increased drop-off across critical appointment flows, and limited the organization’s ability to scale international patient growth safely and sustainably.
Key challenges included:
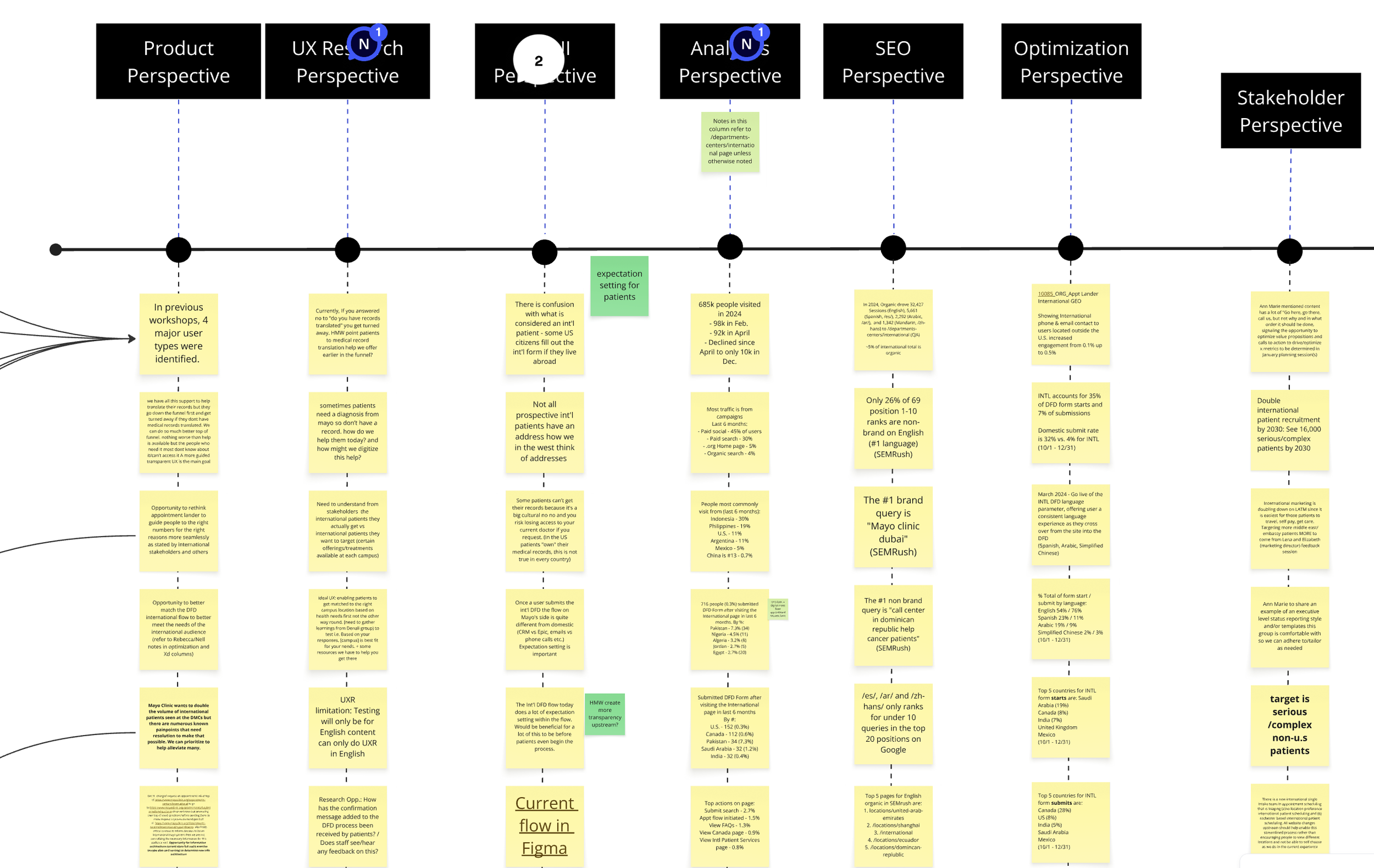
Low discoverability: International pages received less than 5% of traffic from organic search
Misaligned information architecture: Navigation and content structure did not reflect patient mental models or care-seeking behaviors
Fragmented appointment journeys: Redundant steps and unclear terminology caused friction and abandonment
High drop-off at qualification steps: Travel readiness and medical records screens introduced unnecessary cognitive load
Accessibility & compliance risk: Inconsistent standards, particularly across UK pages and forms
Content fragmentation: A separate UK site with thin content weakened clarity, trust, and search authority
Constraints
This initiative operated within several structural and organizational constraints typical of a large, regulated healthcare environment:
Regulatory & compliance requirements: All designs had to meet strict healthcare, accessibility, and regional compliance standards (including UK-specific requirements).
Platform limitations: Work was constrained by existing CMS (AEM) architecture, form frameworks, and shared global components.
Parallel business priorities: Redesign efforts needed to align with ongoing marketing, SEO, and operational initiatives already in flight.
Global audience complexity: Content had to support diverse cultural contexts, languages, and care expectations without fragmenting the experience.
Incremental delivery model: Improvements were shipped iteratively to minimize risk and avoid disruption to live appointment services.
Process & Approach
Phase 1: Foundation & Continuous Discovery (Months 1–3)
Established a dedicated, cross-functional product team
Conducted competitive, gap, and accessibility analyses
Implemented a continuous discovery model with weekly insight cycles
Research methods included A/B testing, card sorting, IA tree testing, qualitative interviews, VOC surveys, and concept validation across priority regions (Canada, Mexico, India, UAE).
Phase 2: Architecture & Content Transformation (Months 4–6)
Rebuilt the IA around real patient mental models and care-seeking behaviors
Consolidated and strengthened UK content to improve clarity and search authority
Content Strategy
Evolved 14 legacy concepts into 20 redesigned pages and 15 net-new pages
Introduced the Tajawal Arabic font to improve legibility and accessibility for Arabic-reading users
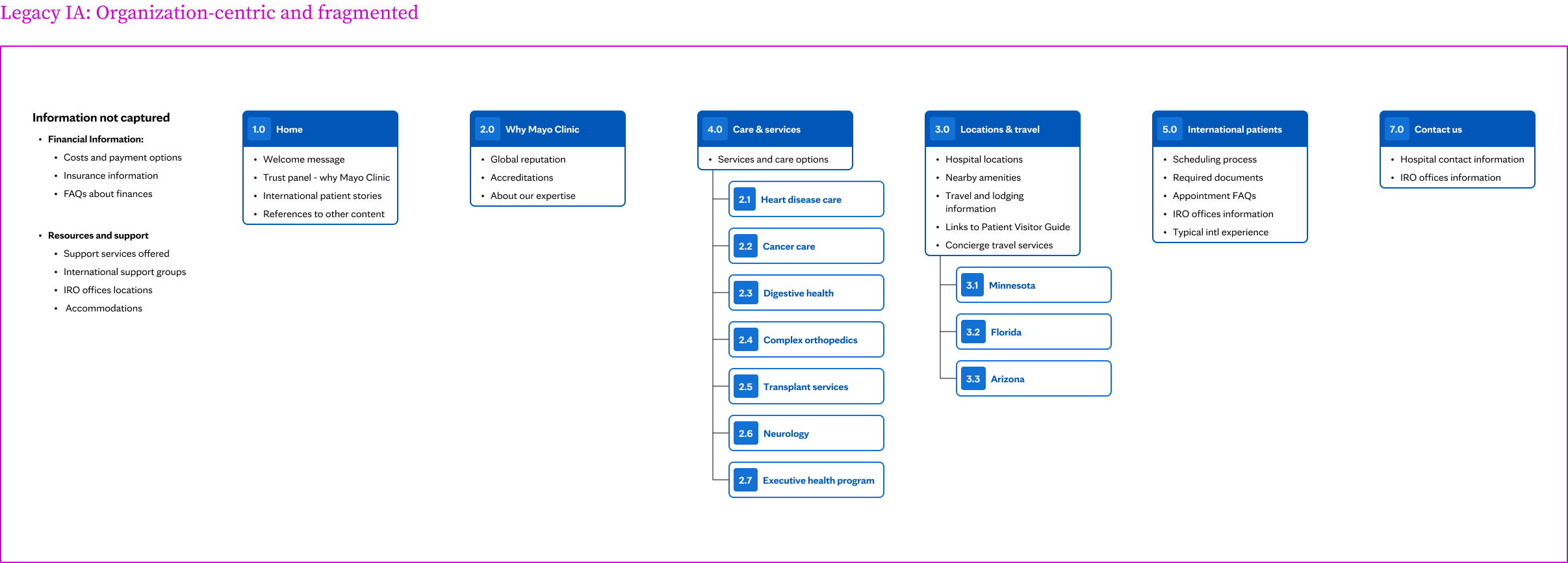
Early research revealed that the legacy IA reflected internal organizational structure rather than international patient decision-making. Patients struggled to understand where to start, how services related to their needs, and what steps were required before requesting care—leading to confusion, misrouting, and drop-off.
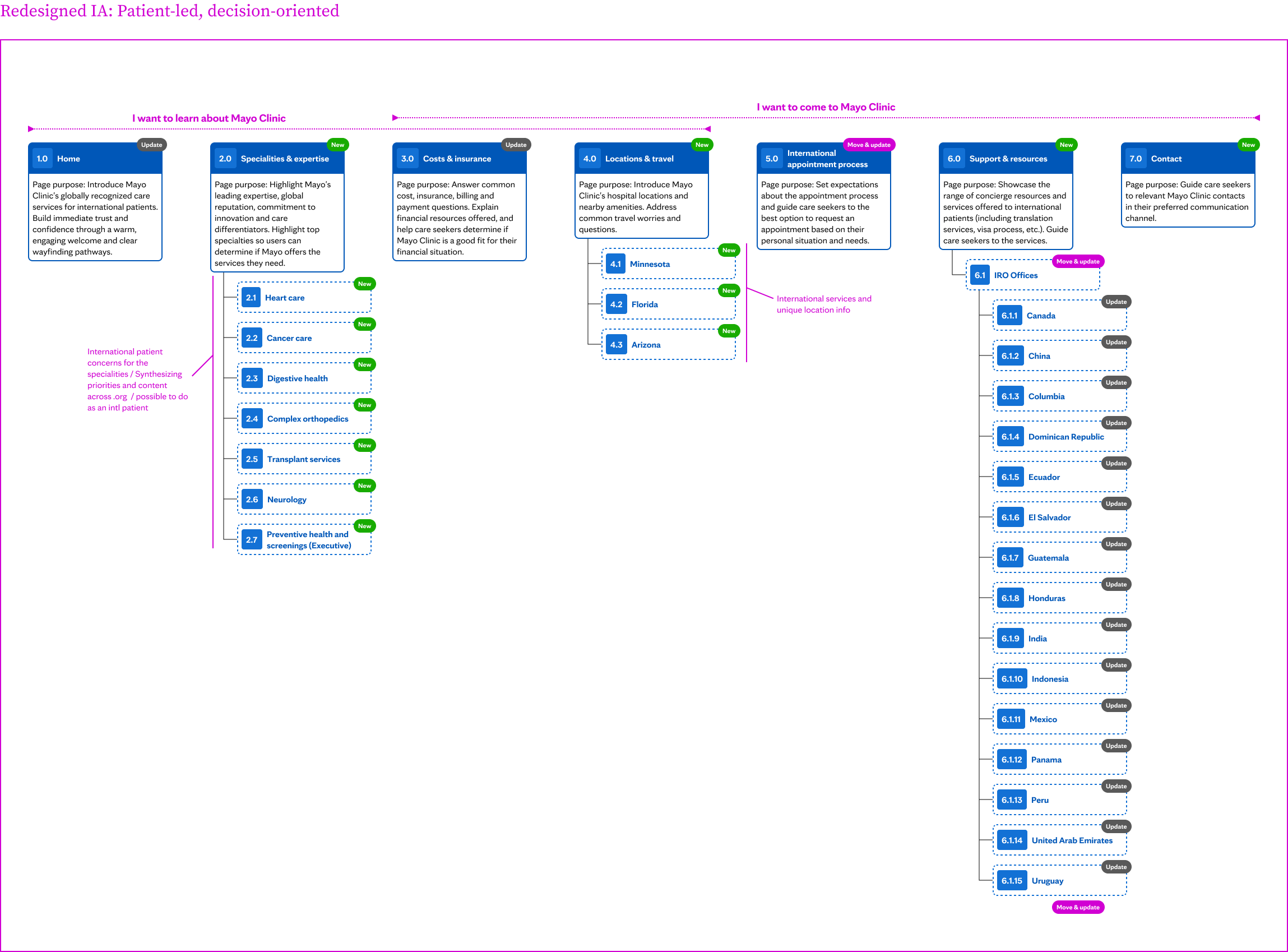
This architectural shift clarified where patients should begin, reduced unnecessary exploration, and aligned content with real care-seeking behaviors. It also improved SEO performance by strengthening topical authority and enabled more intentional self-selection before appointment requests.